
Training itself doesn’t make you better.
When you finish a long run or a set of high-intensity intervals, your body’s capacity actually drops in that moment — muscle micro-damage accumulates, glycogen gets depleted, fatigue builds up. What actually makes you better is the recovery that follows.
Supercompensation: Your Body’s Defensive Upgrade
In 1950, Hans Selye proposed the General Adaptation Syndrome (GAS): the body’s response to stress follows three stages — alarm, resistance, exhaustion. Exercise science borrowed this framework: an appropriate training stress pushes the body into the resistance phase, and after recovery, it doesn’t just return to baseline — it surpasses it.
That “surpassing” is supercompensation.
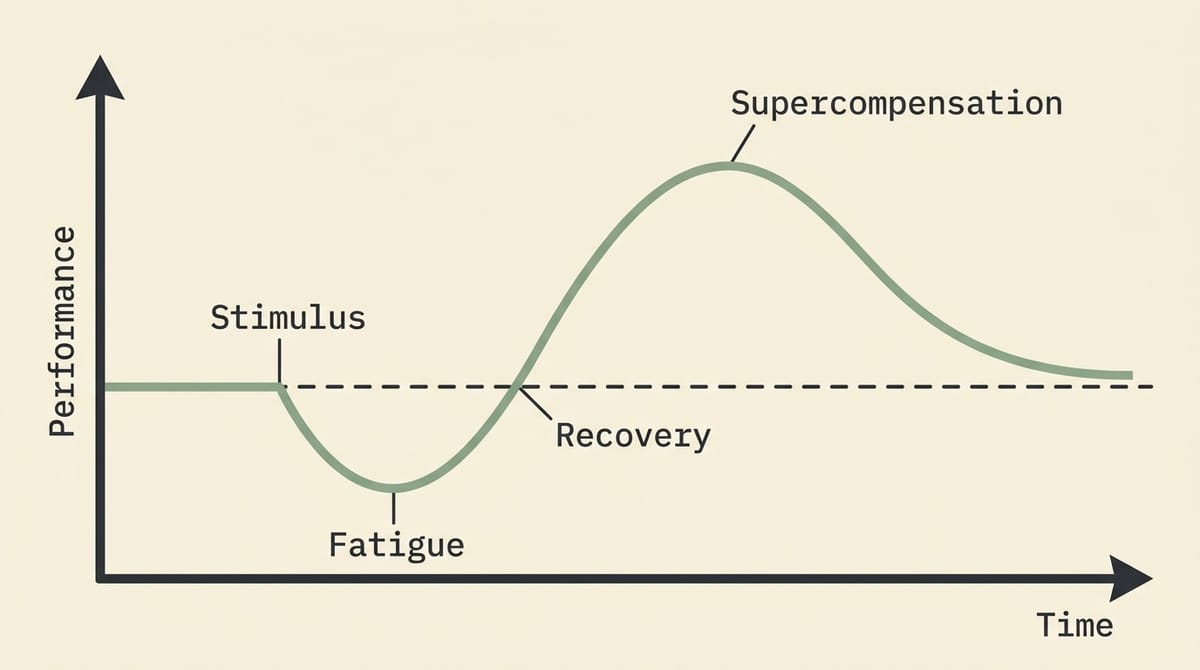
You apply a training stimulus. Your body’s capacity temporarily drops. During recovery, your body rebuilds the damaged structures and “over-repairs” — preparing itself for a stimulus of similar intensity next time. That window of over-repair is when supercompensation occurs. If your next training session lands in this window, you’re applying pressure from a higher baseline, and capacity spirals upward.
The problem: the timing of this window can’t be measured precisely. No device can tell you in real time that “right now is the supercompensation peak, go train.” HRV and resting heart rate are the most practical proxy indicators available, but both have limited precision. This is the biggest practical limitation of the supercompensation model.
Overloading: Forcing the Body to Adapt
The prerequisite for supercompensation is that you’ve given your body a stimulus worth adapting to. That’s the core logic of Overloading.
Overloading means making training stress exceed your current adaptation level, forcing a higher-order adaptation. It’s a tool for progress, not a warning label.
The ACSM’s 2009 resistance training position statement lists the overload variables you can manipulate: load, sets, reps, frequency, movement tempo, rest intervals. “Train more” is not the only way to overload — increasing intensity, shortening rest, or adding frequency are all ways to increase physiological stress without changing total volume.
Training volume (Volume) is itself the primary source of physiological stress. A “smart program” with insufficient training stress has no supercompensation driver; a basic program with sufficient stress and sufficient recovery will still produce adaptation.
The critical point: overloading must advance within the limits of your recovery capacity. When stress accumulates faster than recovery, supercompensation doesn’t happen — instead, you get the next state on the spectrum.
Overreaching: The Line You Only Know You Crossed After the Fact

Overreaching refers to a state where training stress exceeds current recovery capacity, causing a short-term performance decline. The most widely cited classification comes from the 2013 joint consensus statement from the ECSS and ACSM, which organized related states into three tiers [Meeusen et al., 2013]:
Functional Overreaching: Recoverable within days to weeks; capacity typically ends up higher than before training. Elite training cycles often deliberately push into this state in the weeks before competition, then pair it with a taper so supercompensation surfaces before race day.
Non-functional Overreaching: Takes weeks to months to recover. Symptoms go beyond “tired” — hormonal abnormalities appear, with blunted stress responses in growth hormone, ACTH, and prolactin, along with clear deterioration in psychological markers. The training structure has already gone wrong.
Overtraining Syndrome (OTS): Recovery takes months, sometimes more than a year. Multiple systems fail simultaneously — neurological, endocrine, immune. This is a clinical diagnosis, not something that can be self-assessed.
This framework has one fundamental practical problem: the boundary between Functional Overreaching and Non-functional Overreaching is invisible in the moment. All you know is your training load and how tired you feel. Fast recovery gets labeled Functional in retrospect; slow recovery gets labeled Non-functional. There’s no way to know before you start whether today’s training is pushing you past that line.
Halson and Jeukendrup noted as early as 2004 that direct experimental evidence for “overreaching necessarily precedes overtraining” is lacking [Halson & Jeukendrup, 2004]. The spectrum model’s boundaries have never been sharp in practice.
Press Harder, Bounce Higher — This Intuition Is Wrong
If Functional Overreaching paired with a taper brings out supercompensation, is pushing deeper always better?
In 2014, Aubry et al. answered this directly with an experiment [Aubry et al., 2014]. 33 trained male triathletes were split into a normal training group and an overtraining group. Within the overtraining group, 11 were confirmed to have reached Functional Overreaching; the other 12 only reached Acute Fatigue. All subjects then completed a four-week taper.
Results: The Acute Fatigue group showed a supercompensation gain of 2.6% (± 1.1%); the normal training group showed 2.6% (± 1.6%) — similar magnitudes, but the Acute Fatigue group was more consistent. The Functional Overreaching group showed lower supercompensation than the Acute Fatigue group, and had a 70% upper respiratory infection rate during the taper — compared to roughly 10–20% in the normal training and Acute Fatigue groups.
The optimal pre-taper state is Acute Fatigue, not Overreaching. Crossing that line doesn’t make you bounce higher — it makes your system start to break down.
Overtraining Syndrome: It’s Not Just About Training Too Much
You might think that controlling training volume prevents Non-functional Overreaching or Overtraining Syndrome. That assumption doesn’t hold either.
The EROS research series (Endocrine and Metabolic Responses on Overtraining Syndrome) is the most systematic study of Overtraining Syndrome in recent years. The EROS-DISRUPTORS findings were surprising: between Overtraining Syndrome athletes and healthy athletes, training volume showed no statistically significant difference [Cadegiani & Kater, 2019].
The actual independent trigger for Overtraining Syndrome? Diet.
Insufficient carbohydrate intake, insufficient protein intake, insufficient total caloric intake — these three factors can independently induce Overtraining Syndrome without any change in training volume. The effect of insufficient protein is particularly striking: statistically, each unit of protein deficit corresponds to an odds ratio (OR) of 16.7 for developing Overtraining Syndrome.
Overtraining Syndrome patients show what the authors called “Paradoxical Deconditioning”: their physiological markers don’t resemble athletes — they resemble sedentary individuals. Metabolic rate drops, body fat increases, muscle mass decreases, hormonal responses blunt. They keep training, but the adaptive benefit of that training has completely disappeared.
Not enough sleep: recovery capacity drops. Not enough calories: repair materials run short. High life stress: the same training load creates more effective physiological stress. Volume hasn’t increased, but the denominator of recovery capacity is shrinking — relative stress rises.
What This Means for Training Design
Program design isn’t just about arranging training stimuli — it’s about designing the recovery rhythm. Supercompensation needs both adequate stress and adequate recovery. High weekly intensity without planned recovery days or recovery weeks leaves no space for supercompensation to occur.
Overloading is a conscious choice, not a byproduct of “training hard.” The question isn’t whether to apply stress — it’s how much and how much recovery follows. This is a variable that needs active management.
The Functional Overreaching boundary is unpredictable; conservative accumulation is more reliable than aggressive escalation. Aubry 2014 made it clear: Acute Fatigue is the optimal pre-taper state; pushing into Functional Overreaching is counterproductive — and you can’t tell in the moment which side of the line you’re on.
Overtraining Syndrome risk depends on recovery capacity, which is jointly determined by diet, sleep, and life stress. The same training program produces completely different effective stress loads under different life conditions.
The essence of program design is managing the rhythm of stress within the limits of what recovery can handle. When recovery isn’t designed seriously, training stimuli are just stress accumulation.
It doesn’t matter how polished your program looks. If recovery doesn’t happen, it’s all wasted effort.
References
- 1. Selye, H. (1950). Stress and the general adaptation syndrome. British Medical Journal, 1(4667), 1383–1392.
- 2. Bompa, T. O., & Haff, G. G. (2009). Periodization: Theory and Methodology of Training (5th ed.). Human Kinetics.
- 3. Meeusen, R., Duclos, M., Foster, C., Fry, A., Gleeson, M., Nieman, D., ... & Urhausen, A. (2013). Prevention, diagnosis, and treatment of the overtraining syndrome: Joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Medicine & Science in Sports & Exercise, 45(1), 186–205. ↗
- 4. Halson, S. L., & Jeukendrup, A. E. (2004). Does overtraining exist? An analysis of overreaching and overtraining research. Sports Medicine, 34(14), 967–981. ↗
- 5. Issurin, V. B. (2008). Block periodization versus traditional training theory: A review. Journal of Sports Medicine and Physical Fitness, 48(1), 65–75.
- 6. Kreher, J. B., & Schwartz, J. B. (2012). Overtraining syndrome: A practical guide. Sports Health, 4(2), 128–138. ↗
- 7. Aubry, A., Hausswirth, C., Louis, J., Coutts, A. J., & Le Meur, Y. (2014). Functional overreaching: The key to peak performance during the taper? Medicine & Science in Sports & Exercise, 46(9), 1769–1777. ↗
- 8. Cadegiani, F. A., & Kater, C. E. (2019). Novel causes and consequences of overtraining syndrome: The EROS-DISRUPTORS study. BMC Sports Science, Medicine and Rehabilitation, 11(1), 21. ↗
- 9. Cadegiani, F. A., & Kater, C. E. (2020). Diagnosis of overtraining syndrome: Results of the Endocrine and Metabolic Responses on Overtraining Syndrome study—EROS-DIAGNOSIS. Journal of Sports Medicine, 2020. ↗
- 10. American College of Sports Medicine. (2009). Progression models in resistance training for healthy adults. Medicine & Science in Sports & Exercise, 41(3), 687–708.
- 11. Kenttä, G., & Hassmén, P. (1998). Overtraining and recovery: A conceptual model. Sports Medicine, 26(1), 1–16. ↗
If this article was helpful, feel free to buy me a coffee ☕ and keep me writing.